
Qualitative Health Research
2017, Vol. 27(7) 1060 –1068
© The Author(s) 2016
Reprints and permissions:
sagepub.com/journalsPermissions.nav
DOI: 10.1177/1049732316649160
journals.sagepub.com/home/qhr
Methods
Direct observation has been described as the gold standard
among qualitative data collection techniques (Murphy &
Dingwall, 2007). Observing people in their natural environ-
ment not only avoids problems inherent in self-reported
accounts (Mays & Pope, 1995), but can also reveal insights
not accessible from other data collection methods, such as
structures, processes, and behaviors the interviewed partici-
pants may well be unaware of themselves (Furlong, 2010).
Yet, despite now well-documented advantages of observa-
tion over other forms of qualitative data collection, to date,
observation methods have been underused (Mulhall, 2003;
Walshe, Ewing, & Griffiths, 2012), and interviews remain
the most common form of qualitative inquiry in health care
research settings (Morse, 2003; Phillips, Dwan, Hepworth,
Pearce, & Hall, 2014; Russell et al., 2012). Undertaking
observation, particularly in-depth forms of observation
such as traditional ethnography (Savage, 2000), is often
time-consuming, costly, and practically challenging in
health care settings (Curry, Nembhard, & Bradley, 2009;
Morse, 2003; Savage, 2000; Walshe et al., 2012).
More pragmatic contemporary approaches to observa-
tional research suitable for health settings combine less
intensive observation data collection methods with other
forms of data collection in a case study or other type of
multiple-method design (Hjalmarson, Ahgren, &
Kjölsrud, 2013; Kislov, Walshe, & Harvey, 2012).
Incorporating multiple qualitative methods generates the
opportunity for more complete explanations. However,
the unique value of observation methods in multiple-
methods research has remained largely unexplored. All
too often, such studies are in fact predominantly inter-
view driven, failing to use observation data to their full
potential or not reporting them distinctively (Morgan,
Pullon, & McKinlay, 2015; O’Cathain, Murphy, &
Nicholl, 2008).
The focus of this article is on an observationally driven
approach to case study research the authors adopted
649160QHR
XXX10.1177/1049732316649160Qualitative Health ResearchMorgan et al.
research-article2016
1
University of Otago, Wellington, New Zealand
Corresponding Author:
Sonya J. Morgan, Department of Primary Health Care and General
Practice, University of Otago, Wellington, P.O. Box 7343, Wellington
6242, New Zealand.
Email: [email protected]
Case Study Observational Research: A
Framework for Conducting Case Study
Research Where Observation Data Are
the Focus
Sonya J. Morgan
1
, Susan R. H. Pullon
1
, Lindsay M. Macdonald
1
,
Eileen M. McKinlay
1
, and Ben V. Gray
1
Abstract
Case study research is a comprehensive method that incorporates multiple sources of data to provide detailed
accounts of complex research phenomena in real-life contexts. However, current models of case study research
do not particularly distinguish the unique contribution observation data can make. Observation methods have the
potential to reach beyond other methods that rely largely or solely on self-report. This article describes the distinctive
characteristics of case study observational research, a modified form of Yin’s 2014 model of case study research the
authors used in a study exploring interprofessional collaboration in primary care. In this approach, observation data
are positioned as the central component of the research design. Case study observational research offers a promising
approach for researchers in a wide range of health care settings seeking more complete understandings of complex
topics, where contextual influences are of primary concern. Future research is needed to refine and evaluate the
approach.
Keywords
appreciative inquiry; case studies; case study observational research; health care; interprofessional collaboration;
naturalistic inquiry; New Zealand; observation; primary health care; research design; qualitative

Morgan et al. 1061
during the Study of Interprofessional Practice in Primary
Care (SIPP Study)—a multiple case study designed to
explore interprofessional collaboration (IPC) in primary
care teams in New Zealand. We have coined the term
case study observational research (CSOR) to denote this
as a distinct form of case study research (CSR). The
approach incorporates both non-participant observation
of practice activity and policy documents and the non-
observation method of interviewing. However, CSOR
gives priority and precedence to the collection and analy-
sis of observation data, to better understand complex phe-
nomena, such as IPC.
CSR examines “a contemporary phenomenon in depth
and in its real-world context” (Yin, 2014, p. 237). Multiple
methods are used to collect data for each “case” or sub-
ject of study, which is not the same as mixed-method
research (Morse & Cheek, 2014; Yin, 2014). As a method,
CSOR is specific to CSR design. To place our CSOR
approach in its methodological context, we first provide
an overview of the two key antecedents to the approach:
CSR and observation methods. Second, we describe the
informing philosophical approach and the research set-
ting in which CSOR was developed and finally define the
three distinctive features of the approach.
Overview: Case Study Research and
Observation Method
CSR is a comprehensive method increasingly applied in
health sciences research (Anthony & Jack, 2009; Boblin,
Ireland, Kirkpatrick, & Robertson, 2013; Carolan, Forbat,
& Smith, 2016) to investigate “how” or “why” qualitative
research questions, “when the investigator has little con-
trol over events and when the focus is on a contemporary
phenomenon within some real-life context” (Yin, 1994,
p. 1). In this way, CSR differs from other research meth-
ods, such as experiments, which purposefully separate a
phenomenon from its context. In CSR context is inextri-
cably linked to the phenomena under investigation and,
therefore, is crucial to understanding real-world cases
(Yin, 2014).
Several models of CSR exist, each emphasizing differ-
ent philosophical positions (Abma & Stake, 2014).
Within the health care arena, Yin’s (1994) model is com-
monly described and used. Case studies can include either
single- or multiple-case designs. Depending on the con-
text, multiple cases can provide greater confidence in
findings generated from the overall study (Yin, 2014). A
characteristic feature of CSR, the collection of data using
multiple sources for each case (Carolan et al., 2016),
allows triangulation of evidence. Triangulation improves
the accuracy and completeness of the case study, strength-
ening the credibility of the research findings (Cronin,
2014; Yin, 2014). Sources of data collected vary
depending on the research question. Commonly used
methods include interviews, observation of archival
records, and direct observation of study participants (Yin,
1994).
Either as part of CSR or as a stand-alone method,
observation methods involve directly observing and
recording how research participants behave within and
relate to their physical and social environment as it
unfolds (Mays & Pope, 1995; Mulhall, 2003). Observation
provides “insight into interactions between dyads and
groups; illustrates the whole picture; captures context/
process; and informs about the influence of the physical
environment” (Mulhall, 2003, p. 307). Approaches to
observation vary according to the philosophical orienta-
tion of the research and the role researchers adopt along
the continuum of observer to participant (Walshe et al.,
2012). Observation methods may consist of non-partici-
pant observation, where the researcher has no other rela-
tionship with the group being observed (including
shadowing; Quinlan, 2008) through to participant obser-
vation, where the researcher is also a member of the
group being observed (Bloomer, Cross, Endacott,
O’Connor, & Moss, 2012). Recording methods range
from structured template recording to unstructured field
noting (Walshe et al., 2012). More recently, video-record-
ing techniques have proved a valuable way to capture
observations (Carroll, Iedema, & Kerridge, 2008; Collier,
Phillips, & Iedema, 2015; Cronin, 2014; Forsyth, Carroll,
& Reitano, 2009; Iedema et al., 2009).
Compared with observation methods, non-observation
(self-report) qualitative methods, such as interviews or
focus groups, are typically less challenging to undertake
but are subject to participant reporting problems (Curry
et al., 2009; Morse, 2003; Walshe et al., 2012; see Table 1
for summarized strengths and challenges of observation
vs. self-report methods). Thus, observation methods
stand in a class of their own. Observation allows the
researcher to actually see what people do rather than what
they say they do (Caldwell & Atwal, 2005; Mulhall,
2003; Walshe et al., 2012). Systematically observing peo-
ple in naturally occurring contexts can reveal much more
information than individuals may recall, be aware of,
choose to report, or decide is relevant than with other
self-report data collection methods (Mays & Pope, 1995;
Morse, 2003; Mulhall, 2003).
In a health care context, observation methods enable
the exploration of elements of health care that are not
possible by relying on self-report methods (Oandasan
et al., 2009; Russell et al., 2012), providing insights into
the complexity of clinical practice (Dowell, Macdonald,
Stubbe, Plumridge, & Dew, 2007; Lingard, Reznick,
Espin, Regehr, & De Vito, 2002). For instance, observa-
tion methods have been used to observe various aspects
of the interaction between professionals and patients
1062 Qualitative Health Research 27(7)
during medical consultations (Dowell et al., 2007;
Morgan, 2013). They have also been found to be particu-
larly useful for research involving vulnerable patients
where the least intrusion or stress on participants is
desired (Bloomer et al., 2012; Bloomer, Doman, &
Endacott, 2013; Walshe et al., 2012).
Some well-conducted studies have used observation
methods to examine professional practice and communi-
cation between health professionals such as team func-
tioning/communication in the operating room (Lingard
et al., 2004), ward rounds (Carroll et al., 2008), rehabili-
tation settings (Sinclair, Lingard, & Mohabeer, 2009),
and primary care settings (Oandasan et al., 2009; Russell
et al., 2012). Nonetheless, in many health care research
studies incorporating both observation and other forms of
data collection, the observation data are only mentioned
in passing and are therefore underexploited, often taking
a “back seat” to interview data (Morgan et al., 2015).
Thus, for the study next described, an approach to con-
ducting CSR was required that would combine the
strengths of different methods but specifically prioritize
the observation data.
Development of the CSOR
Framework: The SIPP Study
The SIPP Study conducted in 2012–2014 explored feasi-
ble methods of investigating elements of IPC in primary
care practice (Pullon, Morgan, Macdonald, McKinlay, &
Gray, 2016). CSR (Yin, 2014) was originally selected as
an appropriate method, using a multiple case study
design. IPC is challenging to investigate, and the essen-
tial elements of effective IPC remain obscure (Morgan
et al., 2015). IPC has been described as “an active and
ongoing partnership, often between people from diverse
backgrounds, who work together to solve problems or
provide services” (Barr et al., 2005, as cited in Ødegard,
2006, p. 2). It has been shown to improve patient satisfac-
tion (Proudfoot et al., 2007) and health outcomes (Strasser
et al., 2008), yet IPC is far from integral to everyday
practice (Xyrichis & Lowton, 2008).
At the outset, the research approach drew on both nat-
uralistic inquiry (Lincoln & Guba, 1985) and apprecia-
tive inquiry (Cooperrider & Srivastva, 1987). Naturalistic
inquiry contends that “realities are wholes that cannot be
understood in isolation from their contexts” (Lincoln &
Guba, 1985, p. 39). Consistent with the interpretivist tra-
dition of naturalistic inquiry (Lincoln & Guba, 1985), the
aim of the research was to explore the observed nature of
collaboration between practice team members in context
from multiple perspectives. Appreciative inquiry exam-
ines what works well in an organization and acknowl-
edges but does not focus on problems (Cooperrider &
Srivastva, 1987). Informed by the principles of this
approach, we sought to identify key elements influencing
effective IPC. A secondary aim was to investigate whether
well-established interprofessional competencies devel-
oped in Canada (Canadian Interprofessional Health
Collaborative [CIHC], 2010) were evident in the every-
day practice of primary care teams in a New Zealand con-
text. To extend beyond elements of personal
interprofessional relationships and intrinsic team factors
that have been well captured by numerous interview-
based studies, observation methods were incorporated
from the outset in the design of the research. However, as
conventional case study models, such as Yin (2014), do
not distinguish observation data from other types of data
collection in terms of their unique significance and poten-
tial, we modified Yin’s CSR method. This observation-
ally driven, sequential approach to CSR explicitly
positions the observation data as the central component
of the research design, where observation data are both
collected and analyzed prior to augmenting by other non-
observation methods.
Table 1. Observation Versus Self-Report Data Collection Methods: Strengths and Challenges.
Observation Methods Self-Report Methods
Strengths Challenges Strengths Challenges
Allows direct examination of
behavior/activity in real time
Provides information about
topics participants may
be unwilling to talk about,
unaware of, or unable to recall
Undertaken in naturally
occurring contexts—allows
examination of contextual
factors
Time-consuming, expensive, and
ethically challenging in some
settings
Hawthorne effect—participants
may change their behavior
when they know they are
being observed
a
Field noted/video-recorded
observations are influenced by
what the observer chooses to
record/analyze
Allows participants to describe
their own perceptions and
views about the topic of
interest
Relatively straightforward to
undertake
Relies on the information
participants are willing to talk
about, aware of, or able to
recall
Interview/focus group content is
influenced by the perspective
of the interviewer/other
participants
Does not capture context
a
Landsberger (1958).

Morgan et al. 1063
Study Participants and Data Collection
Three widely diverse general practices in a New Zealand
region were approached to participate in the study and all
agreed to take part, constituting the “cases” included in
the study. The practices were purposively selected on the
premise that they were already successfully engaged in
some interprofessional activity, increasing the potential
learnings from the cases (Cooperrider & Srivastva, 1987;
Lincoln & Guba, 1985). Practices varied with respect to
geographical location, size of enrolled patient population,
business model, ownership/governance, and workforce
composition. Data collection at each practice included
non-participant unstructured observation (Mays & Pope,
1995) of informal practice activity (field notes), meetings
(video-recorded), and policy document review (field
notes). Observation-informed individual semi-structured
interviews (audio-recorded) were undertaken only after
other observation data collection was complete. Consent
to participate in the study and have informal practice
activity observed was obtained from the practice as a
whole following presentation of the proposed study by
the research team at a practice meeting. Staff then indi-
vidually consented to the video-recorded meetings and
interviews (Pullon et al., 2016).
Direct observation of informal staff interactions at
each practice were made by a research nurse with a pro-
fessional background who was both familiar with the rou-
tines and sensitivities of the clinical environment and had
extensive experience collecting naturalistic observation
data in primary care settings. The research nurse had no
prior relationship with the selected practices. Her role and
the purpose of the observations, including the apprecia-
tive nature of the research, were explained to participants
during the initial meeting with the study team. Because
we sought to examine how participants naturally inter-
acted with each other, the research nurse situated herself
unobtrusively in the practice and had limited interaction
with participants. Observations were undertaken in as
many of the “common” areas of the practice as possible,
excluding consulting rooms. They were also undertaken
at different times of the day and week. Consultations with
patients were not observed. Observations recorded were
governed by the research nurse’s interaction with and
growing knowledge of the context. They were not guided
by predefined tools or templates (Lincoln & Guba, 1985).
Observations were recorded initially as handwritten
detailed verbatim field notes with time markers. These
notes were supplemented with post-observation summa-
ries generated immediately following the observation
period and incorporated the research nurse’s reflections
on her own feelings, actions, and responses to the situa-
tions observed (Lincoln & Guba, 1985; Mays & Pope,
1995). These field notes and reflective summaries were
promptly circulated to the research team for review, who
in turn added comments and observations, which were
circulated to all members.
Following observations of informal staff interactions,
practices chose which regular practice meeting would be
video-recorded by the research nurse on two successive
occasions. Different types of meetings were chosen at
each practice (i.e., a small team of three to five members;
a medium sized team of six to 14 members, and a large
team of 15+ members) and included different discipline
mixes. Assurance was given as to secure encrypted stor-
age of video and other data. The research team met regu-
larly to review and discuss the video-recorded meetings,
and selected sequences were transcribed verbatim.
Practice documents (e.g., policies, terms of reference,
floor plans) were viewed and summarized as separate
field notes. Finally, observation-informed interviews
were undertaken with a range of practice staff and tran-
scribed verbatim. Ethical approval was granted by the
University of Otago Health Ethics Committee, CEN/11/
EXP/038.
Data consisted of a total of 32 hours of field-noted
observation of informal practice activity, 6 hours of
video-recorded team meetings, 17 individual interviews
(duration ranging from 24 to 48 minutes), and 43
reviewed documents. To support the process of analysis,
all of these separate items of data, including videos,
were imported into the software program NVivo 9
(Bazeley & Jackson, 2013). Preliminary case-specific
findings were presented back to each participating prac-
tice, and the ensuing discussion further informed and
strengthened the credibility of study findings (Boblin
et al., 2013; Houghton, Casey, Shaw, & Murphy, 2013).
Study results have been reported elsewhere (Pullon
et al., 2016).
The remainder of this article focuses on the three fea-
tures of the CSOR approach that differentiate it from con-
ventional CSR: (a) Observation data are collected prior to
and inform the subsequent collection of non-observation
data, (b) observation data determine the analytic frame-
work, and (c) observation data are explicitly referenced in
the final results. Examples from the SIPP Study are used
to illustrate how following this framework afforded pre-
cedence to the observation data.
Distinctive Features of the CSOR
Framework
The three key characteristics of CSOR differentiate it
from conventional CSR and allow the observation data
to contribute uniquely to the case study findings. The
first difference between traditional CSR and CSOR
emerges when it comes to collecting the case study
evidence.

1064 Qualitative Health Research 27(7)
Observation Data Collected Prior to (and
Inform) the Subsequent Collection of Non-
Observation Data
The collection of multiple sources of evidence is central
to CSR (Yin, 2014). However, advocates such as Yin do
not place any significance or importance on the order in
which different sources of data are collected, and indi-
vidual case studies appear to comprise independent data
sets (e.g., interviews, observations, documents, and sur-
veys) collected in no particular sequence.
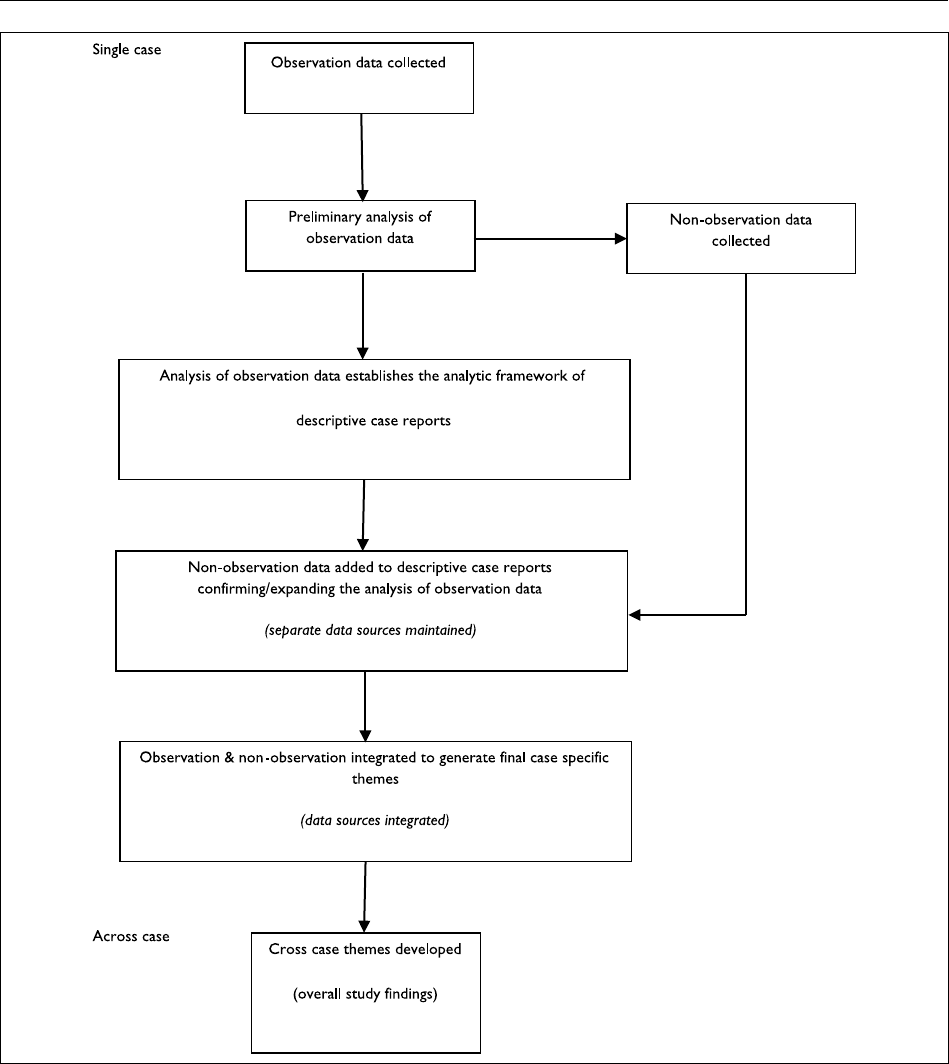
In contrast to conventional CSR, within the CSOR
framework, observation data are analyzed ahead of the
subsequent collection of non-observation data. In this
way, the collection of non-observation data is informed
by the observation data and allows corroboration and fur-
ther exploration of significant observations (Figure 1).
For instance, in the SIPP Study, collecting observations
of health professional interactions prior to undertaking
individual interviews allowed us to consider actual exam-
ples of notable practice team decisions, to explore and
confirm with participants during interviews.
Observation Data Determine the Analytic
Framework
The analysis of case study data is the most difficult and
least developed or described aspect of conventional CSR
(Carolan et al., 2016; Cronin, 2014; Yin, 1994). At a
broad level, consistent with conventional CSR, our CSOR
approach to exploring collaboration in practice teams
involved combining multiple sources of evidence to form
case study conclusions (Yin, 2014). However, in contrast
to conventional approaches, where independently col-
lected sources of data either generate separate findings or
integrate simultaneously in the analysis phase to form
overall case findings (Yin, 2014), CSOR involves an
explicitly sequential approach to analysis (see Figure 1).
A recurring part of the problem with previously pub-
lished research involving multiple methods is that the
interview data governs the framework for the analysis
(Morgan et al., 2015). In contrast, in the SIPP Study, as
recommended by Morse (2010), each of the different
sources of data was initially analyzed and reported sepa-
rately prior to the result-integration phase. However, the
initial analysis stemmed from the observation data as a
stand-alone data set, which then informed interview ques-
tion areas probed during subsequent interviews with indi-
vidual practice team members. The CIHC (2010)
competency framework (including interprofessional
communication, patient-centered care, team functioning,
role clarification, and conflict resolution) was the starting
point that informed the preliminary iterative analysis.
Using an overall inductive process (Lincoln & Guba,
1985), the CIHC framework along with de novo catego-
ries emerging from the observation data (most relating to
contextual influences on IPC) was used to establish the
analytic framework contained within each of the descrip-
tive case reports. Interview transcripts were then exam-
ined to confirm, supplement, and expand on the
observation data in each report.
The descriptive case reports provided a clear chain of
evidence linking the detailed case study findings back to
the different forms of raw data (Yin, 2014). They also iden-
tified similarities as well as potentially important differ-
ences between data sources. In a second level of analysis, a
general thematic analysis of descriptive case reports (Braun
& Clarke, 2006) was undertaken, integrating the observa-
tion and non-observation data to generate the case-specific
themes. Similarities and differences among the case-spe-
cific themes were examined, and overarching cross-case
themes were produced. In the course of this inductive ana-
lytic process, the CIHC framework did not emerge as key
explanatory themes. Using the observation data as the
foundation for the analysis in the SIPP Study revealed new
understandings about key factors influencing effective IPC
that may not have emerged otherwise. Most notably, this
included the importance of contextual/organizational ele-
ments (the built environment, practice location, and busi-
ness models), which fostered opportunities for frequent,
shared informal communication (Pullon et al., 2016).
Observation Data Explicitly Referenced in
Final Results
In the final stage of CSR, adequately reporting the com-
plexity of case findings can be difficult (Baxter & Jack,
2008; Yin, 2014), particularly within the space constraints
of health care journals. As with any qualitative study,
publications ought to reference specific data examples.
This provides readers with the opportunity to examine the
detail and evaluate the chain of evidence to determine
how conclusions have been reached (Rowley, 2002; Yin,
2014). Yet, in most previous research examining IPC in
primary care, referenced examples from observation data
are rare, either not mentioned beyond the methods
description or referred to ambiguously, embedded within
descriptions of the study findings (Morgan et al., 2015).
In contrast, in the reported results of the SIPP Study,
examples have been included from each of the different
data sources and clearly referenced back to the original
field notes or other sources (Pullon et al., 2016). Ensuring
reported findings are explicitly referenced to data sources
in published articles improves the rigor of the research by
not only making the chain of evidence transparent but
also further increasing the likelihood that the reported
findings are not disproportionally represented by self-
reported interview data.
Morgan et al. 1065
Discussion
This article has proposed a new framework, CSOR, for
conducting observationally driven CSR in health care set-
tings. Because of the potential for observation data to
contribute uniquely to research findings, CSOR positions
observation data at the center of the research design:
Observation data are collected prior to and inform the
subsequent collection of non-observation data, and deter-
mine the analytic framework and are explicitly referenced
in the final results. The fundamental assumption of the
approach is that observation is an optimal method for
investigating health care phenomena, which are known to
be difficult to measure, such as IPC, and where the focus
Figure 1. Case study observational research: Sequence of data collection and analysis.

1066 Qualitative Health Research 27(7)
of the research involves examining how people go about
an activity of research interest in a particular naturally
occurring context. The knowledge that observation pro-
vides significant advantages over self-reported forms of
data is not new. However, there is a lack of guiding
frameworks available to inform researchers wishing to
use observation methods in multiple-method studies, in a
way that gives precedence to the observation data.
The key advantage of utilizing a CSOR approach is that
through combining observation with other forms of data
collection in a CSR design that prioritizes the observation
data, a richer understanding of the phenomena of interest
can be achieved. Previous research undertaken in health
care settings has underutilized observation data, resulting in
a predominance of interview-based findings, which appear
to underrepresent wider contextual influences (Morgan
et al., 2015). In our study, using the CSOR framework
revealed important contextual elements influencing effec-
tive IPC in primary care teams that had not previously been
identified from interview-dominated studies.
Collecting and analyzing observation data prior to col-
lecting interview data is a clear strength of the CSOR
approach. This sequential design enabled the research nurse
to focus on enabling the context to “speak for itself.” It also
provided the opportunity to undertake observation-informed
context-specific interviews, revealing important information
that may otherwise have been missed. Yet, this sequential
design is not without limitations. An important potential risk
of using observational findings to inform interviews is that
the interviews may raise ethical issues for participants.
However, this did not appear to be the case in our study
where the selection of observation material discussed during
interviews was enriched by the appreciative inquiry
approach. In addition, as reported by others using similar
qualitative methods in natural settings (Wiles, Coffey,
Robison, & Prosser, 2013), ethical safety in our study was
further improved by developing relationships of mutual trust
with the research participants.
The strength of the sequential design was augmented
by the non-participant observer role adopted, allowing the
research nurse to unobtrusively observe practice teams
from a quasi-“neutral” perspective without any insider
knowledge of how each of the particular teams functioned.
Participant observation, where the researcher is also an
active member of the team, has the advantage of increas-
ing the likelihood participants will behave naturally as the
presence of an outsider can influence behavior. However,
through the feedback from the practice teams involved
and subsequent interviews, we did not find any evidence
of participant discomfort with the observations under-
taken in our study. Our research nurse’s independent role,
along with the appreciative inquiry approach used, is
likely to have facilitated her being readily accepted into
the practices by the research participants. Importantly,
with either type of observer role used, the resulting field
notes must be interpreted as reported accounts of what the
observer chooses to observe and record (Caldwell &
Atwal, 2005), and reflect a mutual influence between the
observer and the observed (Lincoln & Guba, 1985).
CSOR provides an alternative to more complex observa-
tional approaches such as traditional ethnography. Whereas
traditional ethnographers typically enter the field for sus-
tained periods of time without any formally specified
research questions (Cohen & Court, 2003; Roper & Shapira,
2000), CSOR aims to better understand specific complex
naturally occurring phenomena through the examination of
selected cases. However, the unstructured observation com-
ponent of the CSOR approach was still a time-intensive
aspect in our study. Other limitations of the CSOR frame-
work in its current form are recognized in that it is an explor-
atory approach, developed iteratively in the course of a study
investigating IPC in primary care. More research is needed
to further explore and verify the approach. Nonetheless,
CSOR will be of interest to researchers working in a wide
range of health care settings. CSOR is a modified approach
to one form of multiple-method research, CSR. Future
research could explore how to extend the principles of the
approach to other multiple-method research designs.
Conclusion
Health care research incorporating multiple methods would
benefit from more effectively utilizing observation data
because of the potential for direct observation techniques to
contribute unique knowledge and understanding. The CSOR
framework presented in this article is an adapted form of
CSR and is in early stages of development. The CSOR
framework has been referenced by a study investigating IPC
in primary care teams and provides a distinctive approach to
CSR that explicitly prioritizes the observation data through-
out all stages of the research. The approach was well received
by study participants and proved its value, revealing impor-
tant contextual factors influencing effective IPC that had not
previously been identified from interview-based studies.
Case study observational research developed out of a
study undertaken in a primary care context; however, the
principles of this approach are applicable to researchers
working in a wide range of health care settings. In particu-
lar, CSOR appears a promising framework for exploring
complex research topics where contextual issues are of
primary concern.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect
to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support
for the research, authorship, and/or publication of this article:
This study was funded by grants from the University of Otago

Morgan et al. 1067
Research Committee and the New Zealand Lottery Health
Research Council (Grant 313641).
References
Abma, T. A., & Stake, R. E. (2014). Science of the par-
ticular: An advocacy of naturalistic case study in health
research. Qualitative Health Research, 24, 1150–1161.
doi:10.1177/1049732314543196
Anthony, S., & Jack, S. (2009). Qualitative case study method-
ology in nursing research: An integrative review. Journal
of Advanced Nursing, 65, 1171–1181. doi:10.1111/j.1365-
2648.2009.04998.x
Baxter, P., & Jack, S. (2008). Qualitative case study methodol-
ogy: Study design and implementation for novice research-
ers. The Qualitative Report, 13, 544–559. Retrieved from
http://nsuworks.nova.edu/tqr/
Bazeley, P., & Jackson, K. (2013). Qualitative data analysis
with NVivo. London: Sage.
Bloomer, M. J., Cross, W., Endacott, R., O’Connor, M., &
Moss, C. (2012). Qualitative observation in a clinical set-
ting: Challenges at end of life. Nursing & Health Sciences,
14, 25–31. doi:10.1111/j.1442-2018.2011.00653.x
Bloomer, M. J., Doman, M., & Endacott, R. (2013). How
the observed create ethical dilemmas for the observers:
Experiences from studies conducted in clinical settings
in the UK and Australia. Nursing & Health Sciences, 15,
410–414. doi:10.1111/nhs.12052
Boblin, S. L., Ireland, S., Kirkpatrick, H., & Robertson, K.
(2013). Using Stake’s qualitative case study approach
to explore implementation of evidence-based prac-
tice. Qualitative Health Research, 23, 1267–1275.
doi:10.1177/1049732313502128
Braun, V., & Clarke, V. (2006). Using thematic analysis in psy-
chology. Qualitative Research in Psychology, 3, 77–101.
doi:10.1191/1478088706qp063oa
Caldwell, K., & Atwal, A. (2005). Non-participant observation:
Using video tapes to collect data in nursing research. Nurse
Researcher, 13, 42–54. Retrieved from http://journals.rcni.
com/journal/nr
Canadian Interprofessional Health Collaborative. (2010).
A national interprofessional competency frame-
work. Retrieved from http://www.cihc.ca/files/CIHC_
IPCompetencies_Feb1210.pdf
Carolan, C. M., Forbat, L., & Smith, A. (2016). Developing
the DESCARTE Model: The design of case study research
in health care. Qualitative Health Research, 26, 626–639.
doi:10.1177/1049732315602488
Carroll, K., Iedema, R., & Kerridge, R. (2008). Reshaping
ICU ward round practices using video-reflexive eth-
nography. Qualitative Health Research, 18, 380–390.
doi:10.1177/1049732307313430
Cohen, A., & Court, D. (2003). Ethnography and case study:
A comparative analysis. Academic Exchange Quarterly, 7,
283–287.
Collier, A., Phillips, J. L., & Iedema, R. (2015). The mean-
ing of home at the end of life: A video-reflexive eth-
nography study. Palliative Medicine, 29, 695–702.
doi:10.1177/0269216315575677
Cooperrider, D., & Srivastva, S. (1987). Appreciative inquiry in
organizational life. In R. Woodman & W. Pasmore (Eds.),
Research in organizational change and development (pp.
129–169). Greenwich, CT: JAI Press.
Cronin, C. (2014). Using case study research as a rigorous form
of inquiry. Nurse Researcher, 21(5), 19–27. doi:10.7748/
nr.21.5.19.e1240
Curry, L. A., Nembhard, I. M., & Bradley, E. H. (2009).
Qualitative and mixed methods provide unique contribu-
tions to outcomes research. Circulation, 119, 1442–1452.
doi:10.1161/circulationaha.107.742775
Dowell, T., Macdonald, L., Stubbe, M., Plumridge, E., & Dew,
K. (2007). Clinicians at work: What can we learn from
interactions in the consultation? New Zealand Family
Physician, 34, 345–350.
Forsyth, R., Carroll, K., & Reitano, P. (2009). Introduction.
International Journal of Multiple Research Approaches, 3,
214–217. doi:10.1080/18340806.2009.11004911
Furlong, M. (2010). Clear at a distance, jumbled up close:
Observation, immersion and reflection in the process that
is creative research. In P. Liamputtong (Ed.), Research
methods in health: Foundations for evidence-based prac-
tice (pp. 153–169). South Melbourne, Australia: Victoria
Oxford University Press.
Hjalmarson, H. V., Ahgren, B., & Kjölsrud, M. S. (2013).
Developing interprofessional collaboration: A longitudinal
case of secondary prevention for patients with osteoporo-
sis. Journal of Interprofessional Care, 27, 161–170. doi:10.
3109/13561820.2012.724123
Houghton, C., Casey, D., Shaw, D., & Murphy, K. (2013). Rigour
in qualitative case-study research. Nurse Researcher, 20(4),
12–17. doi:10.7748/nr2013.03.20.4.12.e326
Iedema, R., Merrick, E. T., Rajbhandari, D., Gardo, A., Stirling,
A., & Herkes, R. (2009). Viewing the taken-for-granted
from under a different aspect: A video-based method
in pursuit of patient safety. International Journal of
Multiple Research Approaches, 3, 290–301. doi:10.5172/
mra.3.3.290
Kislov, R., Walshe, K., & Harvey, G. (2012). Managing bound-
aries in primary care service improvement: A developmen-
tal approach to communities of practice. Implementation
Science, 7, Article 97. doi:10.1186/1748-5908-7-97
Landsberger, H. A. (1958). Hawthorne revisited: Management
and the worker, its critics, and the developments in human
relations in industry. Ithaca, NY: Cornell University.
Lincoln, Y., & Guba, E. (1985). Naturalistic inquiry. Beverly
Hills, CA: Sage.
Lingard, L., Espin, S., Whyte, S., Regehr, G., Baker, G. R.,
Reznick, R., . . . Grober, E. (2004). Communication fail-
ures in the operating room: An observational classification
of recurrent types and effects. Quality and Safety in Health
Care, 13, 330–334. doi:10.1136/qshc.2003.008425
Lingard, L., Reznick, R., Espin, S., Regehr, G., & De Vito, I.
(2002). Team communications in the operating room: Talk
patterns, sites of tension, and implications for novices.
Academic Medicine, 77, 232–237. doi:10.1097/00001888-
200203000-00013
Mays, N., & Pope, C. (1995). Observational methods in
health care settings. British Medical Journal, 311(6998),
182–184. doi:10.2307/29728110
Morgan, S. (2013). Miscommunication between patients and
general practitioners: Implications for general practice.

1068 Qualitative Health Research 27(7)
Journal of Primary Health Care, 5, 123–128. Retrieved
from https://rnzcgp.org.nz/assets/documents/Publications/
JPHC/June-2013/JPHCOSPMorganJune2013.pdf
Morgan, S., Pullon, S., & McKinlay, E. (2015). Observation
of interprofessional collaborative practice in primary care
teams: An integrative literature review. International
Journal of Nursing Studies, 52, 1217–1230. doi:10.1016/j.
ijnurstu.2015.03.008
Morse, J. M. (2003). Perspectives of the observer and the
observed. Qualitative Health Research, 13, 155–157.
doi:10.1177/1049732302239595
Morse, J. M. (2010). Simultaneous and sequential qualitative
mixed method designs. Qualitative Inquiry, 16, 483–491.
doi:10.1177/1077800410364741
Morse, J. M., & Cheek, J. (2014). Making room for qualita-
tively-driven mixed-method research. Qualitative Health
Research, 24, 3–5. doi:10.1177/1049732313513656
Mulhall, A. (2003). In the field: Notes on observation in qualita-
tive research. Journal of Advanced Nursing, 41, 306–313.
doi:10.1046/j.1365-2648.2003.02514.x
Murphy, E., & Dingwall, R. (2007). Informed consent, antic-
ipatory regulation and ethnographic practice. Social
Science & Medicine, 65, 2223–2234. doi:10.1016/j.socs-
cimed.2007.08.008
Oandasan, I. F., Conn, L. G., Lingard, L., Karim, A., Jakubovicz,
D., Whitehead, C., . . . Reeves, S. (2009). The impact of
space and time on interprofessional teamwork in Canadian
primary health care settings: Implications for health care
reform. Primary Health Care Research & Development,
10, 151–162. doi:10.1017/S1463423609001091
O’Cathain, A., Murphy, E., & Nicholl, J. (2008). The qual-
ity of mixed methods studies in health services research.
Journal of Health Services Research & Policy, 13, 92–98.
doi:10.1258/jhsrp.2007.007074
Ødegard, A. (2006). Exploring perceptions of interprofessional
collaboration in child mental health care. International
Journal of Integrated Care, 6, e25. Retrieved from http://
www.ijic.org/index.php/ijic
Phillips, C. B., Dwan, K., Hepworth, J., Pearce, C., & Hall, S.
(2014). Using qualitative mixed methods to study small
health care organizations while maximising trustworthi-
ness and authenticity. BMC Health Services Research, 14,
Article 559. doi:10.1186/s12913-014-0559-4
Proudfoot, J., Jayasinghe, U. W., Holton, C., Grimm, J., Bubner,
T., Amoroso, C., . . . Harris, M. F. (2007). Team climate
for innovation: What difference does it make in general
practice? International Journal for Quality in Health Care,
19, 164–169. doi:10.1093/intqhc/mzm005
Pullon, S., Morgan, S., Macdonald, L., McKinlay, E., & Gray,
B. (2016). Observation of interprofessional collaboration
in primary care practice: A multiple case study. Manuscript
submitted for publication.
Quinlan, E. (2008). Conspicuous invisibility: Shadowing
as a data collection strategy. Qualitative Inquiry, 14,
1480–1499. doi:10.1177/1077800408318318
Roper, J., & Shapira, J. (2000). Ethnography in nursing
research. Thousand Oaks, CA: Sage.
Rowley, J. (2002). Using case studies in research. Management
Research News, 25, 16–27. doi:10.1108/01409170210782990
Russell, G., Advocat, J., Geneau, R., Farrell, B., Thille, P.,
Ward, N., & Evans, S. (2012). Examining organizational
change in primary care practices: Experiences from using
ethnographic methods. Family Practice, 29, 455–461.
doi:10.1093/fampra/cmr117
Savage, J. (2000). Ethnography and health care. British Medical
Journal, 321, 1400–1402. doi:10.1136/bmj.321.7273.1400
Sinclair, L. B., Lingard, L. A., & Mohabeer, R. N. (2009). What’s
so great about rehabilitation teams? An ethnographic study
of interprofessional collaboration in a rehabilitation unit.
Archives of Physical Medicine and Rehabilitation, 90,
1196–1201. doi:10.1016/j.apmr.2009.01.021
Strasser, D. C., Falconer, J. A., Stevens, A. B., Uomoto, J.
M., Herrin, J., Bowen, S. E., & Burridge, A. B. (2008).
Team training and stroke rehabilitation outcomes: A clus-
ter randomized trial. Archives of Physical Medicine and
Rehabilitation, 89, 10–15. doi:10.1016/j.apmr.2007.08.127
Walshe, C., Ewing, G., & Griffiths, J. (2012). Using obser-
vation as a data collection method to help under-
stand patient and professional roles and actions in
palliative care settings. Palliative Medicine, 26,
1048–1054. doi:10.1177/0269216311432897
Wiles, R., Coffey, A., Robison, J., & Prosser, J. (2013). Ethical
regulation and visual methods: Making visual research
impossible or developing good practice? Sociological
Research Online, 17, 8. doi:10.5153/sro.2274
Xyrichis, A., & Lowton, K. (2008). What fosters or prevents
interprofessional teamworking in primary and community
care? A literature review. International Journal of Nursing
Studies, 45, 140–153. doi:10.1016/j.ijnurstu.2007.01.015
Yin, R. K. (1994). Case study research: Design and methods
(2nd ed.). Thousand Oakes, CA: Sage.
Yin, R. K. (2014). Case study research: Design and methods
(5th ed.). Thousand Oaks, CA: Sage.
Author Biographies
Sonya J. Morgan (MHealSc) is a research fellow in the
Department of Primary Health Care and General Practice at the
University of Otago, Wellington, New Zealand.
Susan R. H. Pullon (MPHC FRNZCGP MBChB) is an associ-
ate professor and the head of the Department of Primary Health
Care and General Practice at the University of Otago,
Wellington, New Zealand.
Lindsay M. Macdonald (MA [App], RN) is a research fellow
in the Department of Primary Health Care and General Practice
at the University of Otago, Wellington, New Zealand.
Eileen M. McKinlay (MA [App], Ad Dip Nurs, RN) is a senior
lecturer in the Department of Primary Health Care and General
Practice at the University of Otago, Wellington, New Zealand.
Ben V. Gray (MBHL, MBChB) is a senior lecturer in the
Department of Primary Health Care and General Practice at the
University of Otago, Wellington, New Zealand.
